

Pooling the risk of old age: the reform plan councils and providers can both live with
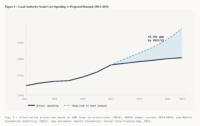
The number of people aged 85 and over in England is on course to double within twenty years. The Office for Budget Responsibility calculates that simply keeping today's care system running will require public spending on social care to rise by 3.1 per cent a year over the next decade, more than four times the 0.7 per cent average managed between 2009/10 and 2022/23. It is, by any measure, a national bill. And yet responsibility for meeting it falls, council by council, on local authorities that have no way to plan for a demographic wave on that scale.
That mismatch is the organising argument of a report published this month by the Care Association Alliance (CAA), the umbrella body for England's independent care providers. Adult Social Care Funding Reform, the first in a planned series and written by lead author William Walter, proposes rebuilding the way England pays for older people's care around a single idea: that the cost of growing old should be pooled nationally, even as care itself continues to be arranged and delivered locally. The plan carries the backing of the Rt Hon Damian Green, chair of the Social Care Foundation and a former deputy prime minister with responsibility for social care.
A system most people misunderstand
Most people assume social care works like the NHS, free at the point of use, available to anyone who needs it. It does not.
Adult social care in England is governed by two tests applied together: a needs test, which restricts publicly funded support to those with substantial or critical needs, and a means test, which restricts it to people whose assets fall below £23,250. Above that line, individuals pay for their own care in full, with no ceiling on what they can be asked to spend.
That £23,250 threshold has been frozen in cash terms since 2010/11. Had it merely tracked inflation, the report notes, it would now stand at roughly £35,118. Because it has not moved, the boundary between self-funding and state support has shifted steadily against families year after year, without any minister ever deciding it should. Research cited in the report found that only around a fifth of the public correctly identified where the threshold sits, or understood what home care actually costs. Most people encounter the rules for the first time in the middle of a crisis.
Behind the means test sits a funding structure that leans heavily on local government. Under the Care Act 2014, primary responsibility for assessing need, commissioning services and managing the provider market rests with 153 local authorities. Total spending on adult social care reached around £34.5 billion in 2024/25, of which councils accounted for £29.4 billion, close to 40 per cent of all local authority service spending, and a share that has climbed as demand has risen and other budgets have been cut. Councils have not squeezed out libraries and road repairs by choice; they carry statutory duties to meet assessed need, and little discretion to do otherwise when money is tight.
The money to discharge those duties has not kept pace. Overall local government spending power remains about 9 per cent below its 2010/11 level in real terms. Council tax now supplies 46 per cent of council income, up from roughly a third in 2010, and the adult social care precept, a ring-fenced council tax add-on, raised £609 million in 2024/25, equivalent to about £32 on a Band D bill. In 2025/26, 350 of 384 councils set council tax at or near the maximum permitted. There is, in short, almost no headroom left in the one lever councils fully control.
What a national bill on local budgets produces
The report's case is that the visible failures of the system are symptoms of that single structural fault, not of bad management. The first symptom is rationing. Only 3.6 per cent of older people now receive local-authority-funded long-term care, and the number of people getting publicly funded long-term support grew by just 2 per cent between 2015/16 and 2024/25, a period in which the older population expanded and complex needs became more common. Access has narrowed not by design but by attrition.
The second is unlimited personal exposure. Because there is no cap on lifetime care costs, and because a private insurance market for care has never developed in Britain, an individual who crosses the asset threshold faces open-ended liability. One in seven people aged 65 can expect to incur lifetime care costs above £100,000, with no public or private mechanism to insure against it.
The third symptom lands on providers. Councils, the report argues, are commissioning care below the cost of delivering it. On average, local authorities pay £24.10 an hour for home care; the Homecare Association puts the minimum sustainable rate at £32.14. The National Audit Office reached the same conclusion in 2021, and the King's Fund found that in 2025/26 council fee increases of around 5 per cent were outstripped by provider cost rises of 8 to 10 per cent, driven by the National Living Wage and higher employer National Insurance. Providers absorb the gap through thinner margins and deferred investment, or through the higher fees paid by self-funders, who on average pay about 41 per cent more than the council rate to subsidise the shortfall. Where that cross-subsidy runs out, provision fails: in 2019, care home closures outpaced openings for an eighth consecutive year, with more than 900 closures against around 600 openings and a net loss of over 23,000 beds. Nearly three-quarters of directors of adult social services reported overspending their care budgets in 2023/24, the highest figure in a decade.
The alternative: a national settlement, delivered locally
Against that diagnosis, the CAA sets out what it calls a national funding settlement, built on three principles. The first is that the financial risk of demographic change should be pooled nationally rather than spread across councils of wildly differing means. The second is that entitlement to support should be established in statute and triggered by assessed need, so that the threshold for help is set nationally and applied consistently, and cannot be quietly raised by a council under budget pressure. The third is that care should continue to be delivered locally, within a national funding and pricing framework rather than absorbed into a centralised, NHS-style service.
In practice the model has five moving parts. A ring-fenced national care grant would be distributed to councils on a needs-adjusted formula, so that funding follows need rather than local fiscal capacity. A reformed means test would raise the frozen capital threshold and, for the first time, impose a lifetime cap on what any individual can be asked to pay. A national tariff for home and residential care would be set at the independently assessed cost of sustainable provision, with councils required to commission at or above it. Residential care would be funded as a single bundled package, portable when a person moves. And a reformed Deferred Payment Agreement scheme would ensure, the report says, that no one is forced to sell their home to pay for residential care.
Holding the structure together would be a new independent National Care Assessment Body, sitting outside both the NHS and local government, tasked with verifying the cost evidence, reviewing the tariff and publishing where provision falls short. Councils, under the plan, keep assessment, planning, safeguarding and market-shaping, but stop being the sole bearers of a national financial risk.
The report is careful about what it is not proposing. This is not free care on the NHS model, and it does not fold social care into the health service. Means-tested contributions remain; the word "national", the authors stress, describes the funding architecture, not the way care is provided.
"No family should receive worse care because of where they happen to live, and no provider should have to choose between keeping a contract and delivering care safely," said Melanie Weatherley MBE, the CAA's co-chair. "These are not failings of the people running the system. They are what happens when a national risk is carried on local budgets." She was at pains to add that the paper "is not a criticism of local authorities, who are doing a demanding job under real pressure."
The postcode lottery, laid bare
If the argument that structure trumps effort needs a single proof, the report offers one: what happens to identical rules in neighbouring places. Once spending is adjusted for the age profile of each area's population, council spend on adult social care runs nationally from £392 per person in Warrington to £991 in the tiny Isles of Scilly. Set that outlier aside and the sharpest like-for-like contrast is Warrington against Knowsley, £392 against £960, a gap of more than two to one between two authorities in the same region, barely twenty miles apart, operating under exactly the same law.
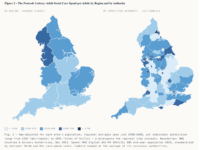
Crucially, the widest gaps open up within regions rather than between them. Age-adjusted regional averages differ by just £108 per person; within the North West alone the spread is £568. The variation, in other words, is not a familiar north–south or rich–poor story. It is local, and it is everywhere.
The report goes further, arguing through a regression analysis that even after controlling for age, deprivation and the local cost of care, somewhere between 55 and 66 per cent of the difference between councils remains unexplained (the analysis, and the age-standardisation method behind the Warrington and Knowsley figures, are set out in the paper's appendices). That is the CAA's own modelling rather than an independent finding, and it rests on data the authors acknowledge is not published at the level of individual council commissioning rates. But the headline pattern (comparable places spending very different sums under the same rules) is not seriously in dispute.

A race to the bottom on standards
The report ties that disparity back to below-cost commissioning, and issues its bluntest warning here. When a council sets a rate beneath the cost of safe delivery, it argues, good providers cannot both win the contract and remain viable; they either walk away or cut corners to survive, and nothing in the current system prevents a rate being set below cost in the first place. The CAA characterises this as a "race to the bottom" on standards, a claim that turns a story about spending variation into one about the quality and safety of care people actually receive.
That framing will not be universally welcomed. Councils have long argued that the real culprit is a decade of constrained funding settlements rather than their own commissioning choices.
Why now?
The timing is deliberate. Baroness Casey used a BBC Radio 4 interview and a speech to the Local Government Association's conference on 7 July to confirm that her commission into adult social care will begin testing public opinion this month (on who should receive care, what the state should guarantee and what individuals should contribute) ahead of a first report due later this year. The CAA has pitched its paper explicitly as a contribution to that process, arguing that funding reform is the necessary first step.
History gives the Alliance reason to press. The report tallies four missed attempts at exactly this kind of change: the Dilnot Commission's recommendations in 2011; the cap and higher capital limit legislated in the Care Act 2014 but never implemented; and a further cap, legislated in the Health and Care Act 2022, that was scrapped by the Treasury in July 2024 to save £1.1 billion. Each deferral, the report argues, has let the means test erode further, the provider market weaken and the funding gap widen.
"The case for reform is no longer contested," said Damian Green. "The case for delay is indefensible. This paper gives the next prime minister, and the Casey Commission, a practical, affordable blueprint, and a cross-party route to deliver it."
The demographic bill, on the CAA's telling, is coming either way. The only real question is whether England chooses to meet it by design, or goes on absorbing it, as now, through a frozen threshold, a provider's thinning margin, and the accident of a postcode.
-
Read the report here: https://www.bridgeheadcommunic...
View the interactive storyboard here: https://www.bridgeheadcommunic...
Eleanor Thomas is a writer for Comment Central.



